
Glaucoma – the proper pronunciation is glaw-koh-muh, but many will come up with their own way of saying it. No, it has nothing to do with guns, glowing, or glue. It actually isn’t completely understood at this time. What you do need to know about it is that it can cause severe permanent vision loss if left untreated. It is a silent thief of vision – as many eye diseases usually are. January was glaucoma awareness month, so I thought it’d be appropriate to shed some light on this condition.
What we do understand about glaucoma, is that it is one of the leading causes of blindness in Canada. Vision loss occurs through a gradual loss of nerve tissue that is irreversible. Although the precise cause is still unknown, it is generally associated with the pressure within the eye being too high for the optic nerve (where all the nerves come together and connect the eye to the brain – passage of information) to handle.
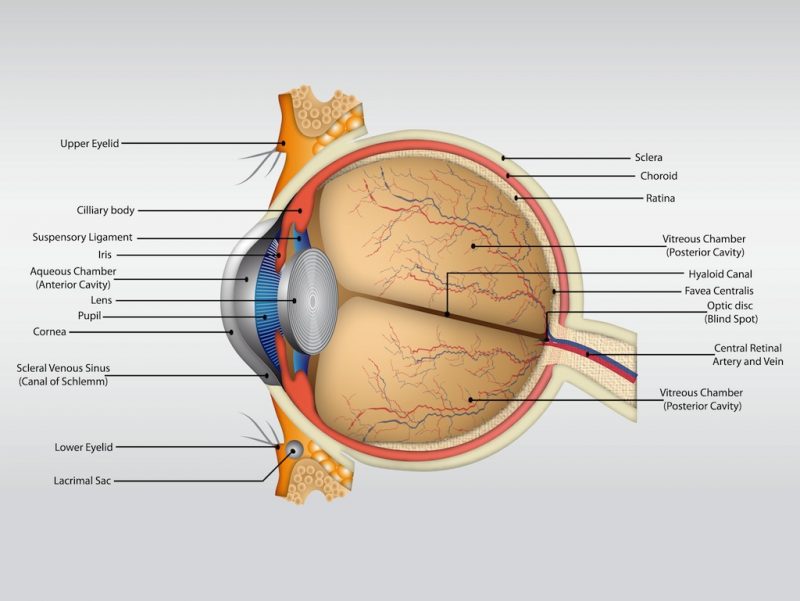
The pressure within the eye is regulated on it’s own and is not directly related to blood pressure. The eye is constantly producing a fluid within the eye called the aqueous humour. This fluid supplies the eye with the nutrients it needs as majority of the structures within the eye are avascular (containing no blood vessels). As this fluid is produced, it also needs to be drained – otherwise the pressure will continually increase. For people that have glaucoma, sometimes this drainage system is not functioning at a high enough capacity to keep up with the production; causing a pressure increase or is faulty. If the optic nerve is not able to handle this pressure increase, there is damage done and nerve tissue lost. This is what causes the gradual vision loss. Peripheral vision is usually lost first before affecting central vision (opposite of macular degeneration).
Pressure increases within the eye are not something we can feel or see unless it spikes up extremely high – then one may experience a combination of the following or only some: severe eye pain, nausea, vomiting, headache, tearing, and blurry vision (may have haloes). This is why it is important to have your eyes checked on a regular basis to ensure the pressure that is being maintained in your eye is healthy for your optic nerve. Although there is a normal range of pressure values, what matters is if your optic nerve can handle the pressure being exerted on it – whether that value is considered normal or not.
Optic nerve physiology is also an important factor in glaucoma and needs to be assessed by an optometrist or ophthalmologist to determine whether or not it appears risky or not. With the help of OCT (optical coherence topography) technology, we are able to look more in depth at the optic nerve and determine if there is tissue loss over time with repeated testing.

With on-going research, we are slowly understanding more about glaucoma and how it works. For now, first-line treatment is drop therapy to control the eye pressure and bring it down to a value the optic nerve can handle. Surgery to open up the drainage system is an option as well and often used in tandem with drops or when drops are not effective. The best way to detect and deal with glaucoma is still with regular eye exams (at least every 2 years and every 1 if risk-factors are identified).